SPIKE trials
The studies by Hoffman et al. (2020) and Yamamoto et al. (2016) have shown that camostat and nafamostat can inhibit the enzyme, TMPRSS2, that hinders the ability of the COVID-19 virus to infect the cell and this can contribute to the slower proliferation of the virus in the human body. Both drugs were developed in Japan in the early 1980s and are still in use to treat chronic pancreatitis and post-operative reflux esophagitis.
In addition, an independent study led by Junichiro Inoue, Professor at the University of Tokyo's Institute of Medical Science, discovered that the drug, nafamostat, is able to block the coronavirus from entering human cells and then inhibit proliferation.
Long-term solution
-
A vaccine against SARS-CoV-2 is the best option
-
However, time is the bottleneck for vaccine development - min of 12 to 18 months is needed
Immediate solution
-
Camostat and Nafamostat are promising off-patent drugs shown to be effective to prevent COVID-19 from infecting host cells. Thus, these drugs are an immediate solution to treat COVID-19 infected patients, via oral and IV formulations.
Immediate solution to treat SARS-CoV-2 patients
In order for SARS-CoV-2 (COVID-19) to be able to infect the human body, it has to bind to its receptor, ACE2, which is present on the cell surface. Then, the fusion of the outer membrane of the virus and the cell membrane must occur.
Once the COVID-19 is bounded to its ACE2 receptor on the cell membrane of human cells, then the TMPRSS2, cleaved by the proteolytic enzyme, must prime S protein to facilitate its activation and enable the fusion.
How SARS-CoV-2 infects the human body
Camostat
-
Camostat is an off-patent, developed by Ono Pharmaceutical in Japan in 1985, and still in use for chronic pancreatitis and Postoperative reflux esophagitis
Nafamostat
-
Nafamostat is an off-patent, developed by Nichi-Iko Pharmaceutical in Japan in 1986, and still in use for chronic pancreatitis and Postoperative reflux esophagitis
Lessons learned from MERS-CoV
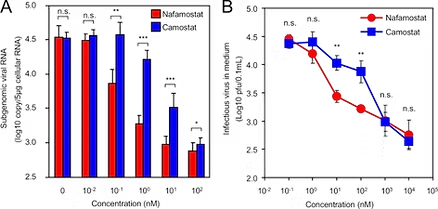
Nafamostat and Camostat are identified from a high-throughput screen of inhibitors against S-mediated membrane fusion of >1000 FDA-approved drugs
Nafamostat decreases membrane fusion for the MERS-S protein to 1.66% of control DMSO
Nafamostat and Camostat showed strong inhibition of MER-S-mediated membrane fusion
SARS-CoV-2 uses ACE2 to enter the host cell
SARS-CoV-2 employs the same receptor as SARS-CoV, for host cell entry: this is due to highly conserved receptor-binding motif (RBM) which facilitates contact with ACE2 receptor.
Hoffmann et al., (2020) confirms that SARS-CoV-2 uses the host ACE2 receptor and not alternative pathways to enter the cell
TMPRSS2 priming required for SARS-CoV-2 entry
Camostat significantly reduces TMPRSS2-dependent coronavirus entry in lung cells
Lung cells (Calu-3)
Primary human lung cells
Nafamostat & Camostat’s
Therapeutic potential for SARS-CoV-2
In Calu-3 cells both Nafamostat and Camostat inhibits MERS-S-mediated membrane fusion.
Nafamostat reduced viral burden by 100-fold at a concentration of as low as 1nM.